Join the Newsletter
Hair transplantation is no longer confined to the scalp. Over the last two decades, eyebrow and beard transplantation have matured into well-established procedures for selected men and women. This article explains why patients seek facial hair restoration, the anatomy and aesthetics involved, how the procedures are performed, who is a good candidate, and where caution is warranted to ensure that precious donor hair is used judiciously.
![[headshot]](https://cdn.prod.website-files.com/68207da82e5b8c350c67932f/68c6a7436a552c0fe87a4da7_Screenshot%202024-11-27%20at%2011.38.11.png)
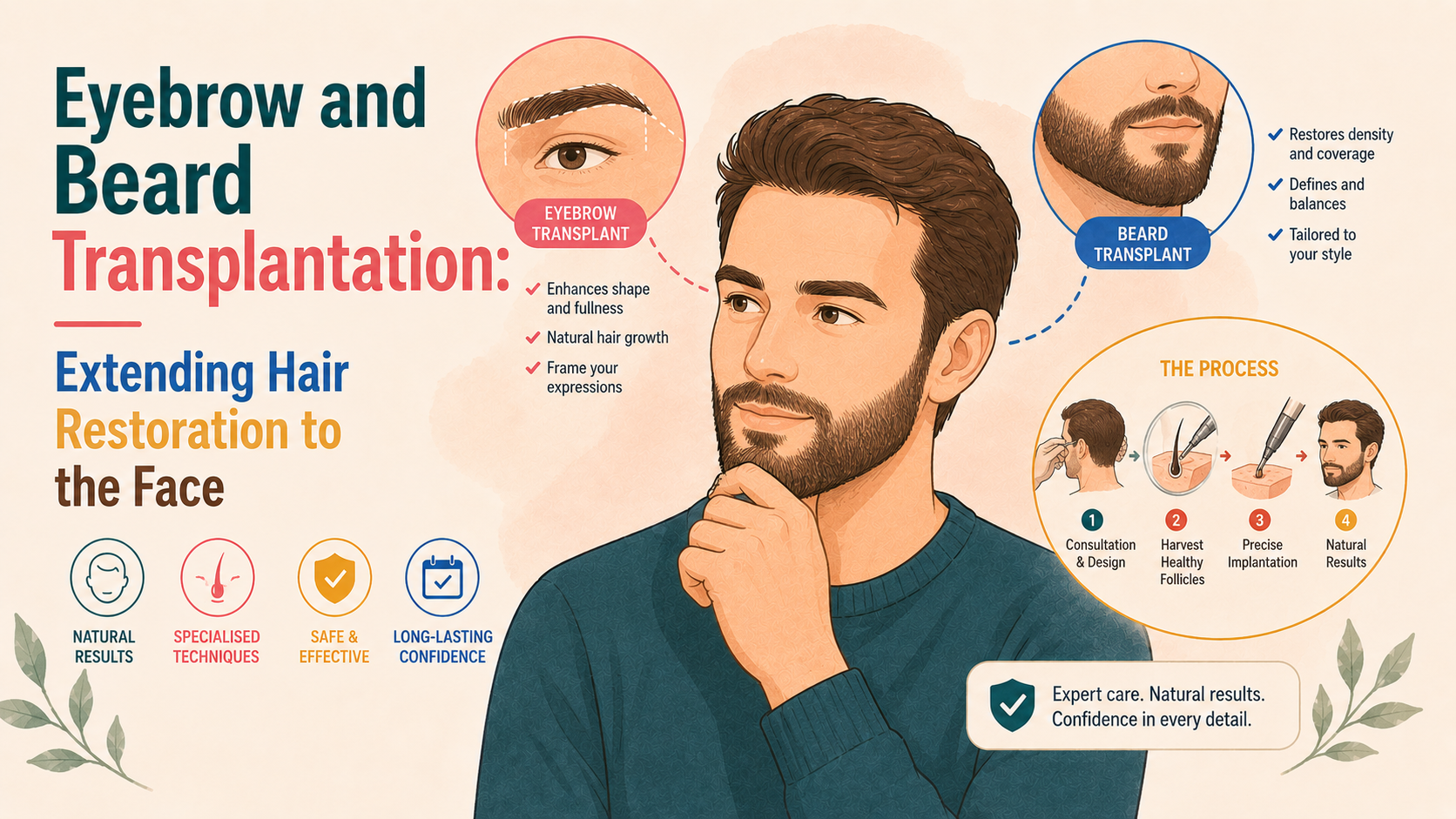
Eyebrows and beards are not simply decorative. They frame the face and play a disproportionate role in non-verbal communication and perceived identity.
Eyebrows contribute strongly to expression, symmetry and gender cues. Their absence or distortion can make the face look “unfinished”, tired, or oddly blank.
Beards and moustaches are, in many cultures, markers of maturity, masculinity and style. Patchy or absent facial hair can be a source of self-consciousness for some men, and beards also play a role in gender affirmation for some transmasculine patients.
Eyebrow and beard loss may follow:
As hair transplant techniques have become more refined, it has become possible to reconstruct these areas with a high degree of naturalness, provided that anatomy, artistry, and donor limitations are respected.
Common reasons for eyebrow transplantation include:
As with scalp transplantation, underlying disease should be stabilised and treated medically before surgery is entertained.
Natural eyebrows have three main parts: a head (medial portion), a body (mid portion), and a tail (lateral portion), with the direction and angulation of the hairs changing subtly across these zones.
The hairs lie very flat against the skin, often at just 5 to 10 degrees from the surface. They point medially at the head, then upward and laterally in the body, and finally downward along the tail. They overlap, creating a soft, feathered border rather than a sharp line.
Eyebrow design, therefore, requires careful mapping of the patient’s facial proportions, respect for gendered patterns (for example, straighter, flatter brows in many men and more arched shapes in many women), and attention to ethnic norms.
Procedures that ignore these subtleties often create “stamped-on” looking brows that draw more attention than the original deficit.
For eyebrow restoration, donor hair is usually taken from the scalp, most often from the mid occipital region, where the hair is finer and closer to natural eyebrow calibre, and occasionally from the temporal region, which provides naturally finer strands.
Because scalp hair tends to grow in follicular units that contain multiple hairs, while eyebrow hairs usually emerge as single strands, grafts are typically harvested using FUE with small punches or with a small strip using FUT, and then dissected under magnification into single hair grafts.
Implantation is done with very small blades, needles or implanters, placing each graft:
Post-operatively:
Because scalp hair is programmed to grow longer than eyebrow hair, transplanted brows need regular trimming every one to two weeks. They may require gentle training with gel or wax in the early months, and they sometimes change in calibre and wave over time, becoming slightly more eyebrow-like.
Published series in the literature report high satisfaction rates, with 80-90% of patients rating their outcomes as good or very good, along with improvements in self-confidence, particularly in those with visible scars or long-standing absence, and low rates of serious complications when cases are carefully selected.
Potential problems include:
These are largely technical issues and emphasise the need for a surgeon experienced in facial hair work, not just scalp.
Beard transplantation has grown rapidly in popularity. Drivers include:
In many settings, beards have become a prominent style feature, and men who cannot grow them may feel out of step with their peers.
Beards vary by culture and preference, but there are recurrent aesthetic principles:
Preoperative planning includes determining the intended facial hair style, such as stubble, a full beard or a goatee. It also involves assessing whether a full beard is in proportion to the patient’s facial structure and evaluating how much donor hair is realistically available.
Donor hair for beards can come from scalp hair (most common) or, in selected cases, from areas of the beard with higher density.
Scalp hair is often a bit finer and blends well, but it tends to grow faster than natural beard hair and may require more frequent trimming.
Beard hair used as a donor (via FUE), usually from under the jawline, has the advantage of matching the recipient's texture exactly but is limited in quantity and must be harvested conservatively to avoid visible thinness.
Implantation is almost always performed using FUE-harvested follicular units. It typically uses 1–2 hair grafts placed at angles that mimic natural growth in each area and requires careful attention to hair direction, especially around the curves of the jaw, chin, and moustache regions.
Graft numbers vary widely, from a few hundred for defining a goatee to 2,000–3,000 or more for a near-complete beard reconstruction.
After a beard transplant, crusting and swelling typically resolve within 1–2 weeks. The transplanted hairs then shed, with new growth usually beginning around three months. Full maturation of the beard generally takes 9–12 months.
Most men report high satisfaction with coverage and styling options, but they also need regular trimming and shaping, since transplanted hair grows at a rate similar to scalp hair. Many also experience a substantial psychological benefit, particularly in gender-affirming cases.
Complications include misdirection, cobblestoning (if slits are too large or shallow), ingrown hairs and, rarely, folliculitis. Again, these are heavily technique-dependent.
Eyebrow and beard transplantation frequently intersect with scarring or inflammatory conditions.
In frontal fibrosing alopecia and lichen planopilaris, the eyebrows and beard can be involved early. Inflammatory destruction of follicles and perifollicular fibrosis may continue to progress.
Transplanting into active disease is risky: graft survival may be poor, transplanted hairs may later succumb to the same process, and surgery itself may provoke flares in some cases.
Most experts therefore recommend only considering transplantation after documented clinical and, ideally, histological quiescence for at least one to two years; continuing medical therapy (for example, hydroxychloroquine or topical calcineurin inhibitors) before and after surgery; and using conservative grafting, with the understanding that additional procedures may be needed.
FFA-related eyebrow loss is particularly tricky; some patients do well with SMP or cosmetic tattooing instead of, or before, surgical eyebrow transplantation.
In alopecia areata, patchy loss in the brows and beard is common, and the disease course is unpredictable.
Transplanting into a diseased area that may reactivate can result in loss of the transplanted hairs and can make subsequent medical therapy more complex.
Transplantation is generally only considered in highly selected cases where the disease has been inactive for several years, where there is a compelling psychosocial need, and where the patient understands and accepts the risk of recurrence.
Often, non-surgical camouflage, such as microblading for the brows and scalp micropigmentation (SMP) for the beard, is a better early intervention.
Eyebrow and beard transplantation often yield excellent results in the following situations: linear scars from cleft lip repair, facial surgery, or trauma; stable burn scars with adequate vascularity; and post-traumatic alopecia.
Graft survival can be lower in dense scars; therefore, test sessions or staging are sometimes used.
Combining surgery with scalp micropigmentation (SMP) or cosmetic tattooing often produces the most natural overall effect.
Every graft placed in an eyebrow or beard is a graft that cannot be used on the scalp. This is particularly important for younger men who are at risk of future extensive androgenetic alopecia, for women with evolving female pattern hair loss, and for anyone with limited scalp donor density.
A thoughtful approach considers:
For example:
The fact that eyebrow and beard transplantation are technically possible does not mean they are always strategically wise.
Scalp micropigmentation and cosmetic tattooing sit alongside transplantation in facial hair restoration.
These methods have inherent risks (colour shift, fading, the need for touch-ups, and technical errors), but they are reversible to a greater extent than poorly placed grafts and preserve the donor site.
Often, the best results come from combinations: subtle SMP plus a beard transplant, or microblading combined with a limited number of eyebrow grafts in key areas.
Facial hair transplantation demands technical skill in FUE or FUT, an understanding of facial aesthetics, and familiarity with how transplanted hair behaves in delicate areas.
When considering eyebrow or beard transplantation, useful questions to ask include:
A surgeon or clinic whose practice is overwhelmingly scalp-focused and who offers facial hair work as an occasional add-on may not be the right fit for complex reconstruction.
Equally, a practitioner who emphasises only the aesthetic end result without discussing donor conservation or underlying disease is not offering a complete picture.