Join the Newsletter
Hormones have a powerful but often misunderstood influence on hair. This article explains how changes in androgens, female sex hormones, thyroid hormones and other endocrine signals can contribute to hair loss, and how doctors approach the evaluation of “hormonal” hair concerns.
![[headshot]](https://cdn.prod.website-files.com/68207da82e5b8c350c67932f/68c6a7436a552c0fe87a4da7_Screenshot%202024-11-27%20at%2011.38.11.png)
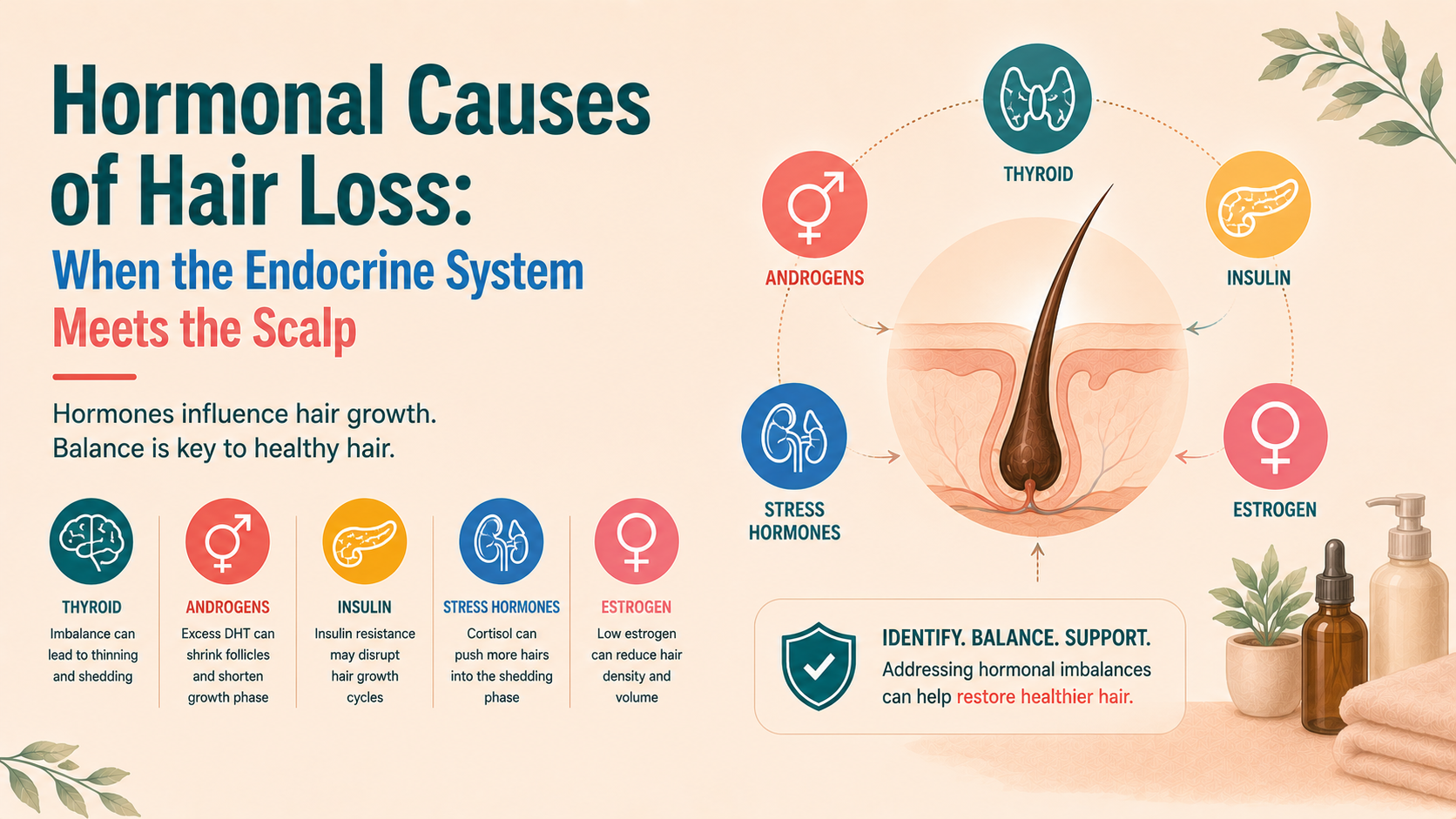
Hair follicles are not separate from the rest of the body. They sit within a web of blood supply, nerves, immune signals and hormones. Several hormones:
Androgenetic alopecia (male- and female-pattern hair loss) is the most common example of hormonal influence, driven by how hair follicles respond to androgens. But it is not the only one. Thyroid hormones, prolactin, cortisol, and metabolic hormones can also influence hair behaviour.
Understanding this does not mean every case of hair loss is “hormonal” in the simplistic sense. It does, however, explain why good assessment considers the person as a whole rather than treating the scalp in isolation.
In both men and women, androgens (primarily testosterone and its more potent derivative, dihydrotestosterone or DHT) play a central part in pattern hair loss.
Crucially, many individuals with androgenetic alopecia have normal systemic androgen levels. The key lies in:
In some women, pattern hair loss occurs in the context of polycystic ovary syndrome (PCOS) or other states of hyperandrogenism.
Features may include:
In these settings, circulating androgens may be elevated or normal, but follicular exposure and sensitivity are often higher. Androgenetic alopecia in women with PCOS may present earlier or progress more rapidly, particularly through the mid-scalp. Management then needs to address both the hair and the underlying endocrine and metabolic issues.
During pregnancy, high oestrogen levels tend to keep a higher proportion of follicles in anagen. Consequently, many women notice thicker, fuller hair and less shedding, because the hair cycle is “held” in a more anagen-dominant state.
After birth, when oestrogen levels fall, this support is withdrawn. A larger number of follicles enter telogen together and shed a few months later – the classic postpartum telogen effluvium. This is usually self-limiting, though in some women it may reveal an underlying tendency toward female-pattern hair loss.
Around perimenopause and menopause:
This does not mean menopause “causes baldness”, but it often brings a pre-existing susceptibility into clearer view. The follicles that were already relatively androgen sensitive have less opposing oestrogenic influence and can therefore drift more quickly towards miniaturisation.
Hormonal contraceptives and menopausal hormone therapies can influence hair in both directions:
These decisions are rarely about hair alone, but the scalp can serve as an indicator of how the hormonal environment is shifting.
Thyroid hormones regulate metabolic activity in many tissues, including the skin and hair follicles. Both hypothyroidism and hyperthyroidism can alter hair cycling and quality.
In low thyroid states, patients may notice:
Follicles tend to have a reduced turnover and can show an increased proportion in telogen. Correcting hypothyroidism usually improves shedding and hair quality, although several cycles may be needed before the change is obvious.
Excess thyroid hormone can also trigger shedding as an increased proportion of follicles may enter telogen. In addition, metabolic demands and systemic stress rise, which can contribute to telogen effluvium.
As with hypothyroidism, the primary treatment is to normalise thyroid function. Hair usually follows suit once the systemic imbalance is controlled.
Routine thyroid testing is not necessary in every case of hair loss, but when there are matching symptoms (weight change, temperature intolerance, palpitations, bowel changes), it is a sensible part of the work-up.
Prolactin is primarily responsible for breast tissue development and milk production after pregnancy, with some additional roles in metabolism and immune function.
Raised prolactin levels (hyperprolactinaemia) can contribute to hair loss, often in concert with menstrual irregularities, galactorrhoea (abnormal milk discharge from nipples) or pituitary pathology. Prolactin interacts with other endocrine axes, and marked elevations may indirectly disturb the hair cycle.
Cortisol is the main hormone associated with the physiological stress response:
The relationship between stress and hair is sometimes overstated, but sustained stress states can certainly tip borderline follicles into a less favourable rhythm.
The hair follicle is responsive to insulin and insulin-like growth factor 1 (IGF-1). Insulin resistance and metabolic syndrome have been associated with more severe androgenetic alopecia in some studies, possibly through:
While not purely “hormonal” in the narrow endocrinology sense, these metabolic signals influence the environment in which follicles operate.
Not every patient with thinning hair needs an exhaustive endocrine work-up. Good judgement lies in matching the investigation to the story.
A typical approach might include:
Not every patient needs every test. Commonly considered investigations include:
The aim is not to find any abnormality at all, but to identify meaningful, treatable hormonal contributors and to distinguish these from the intrinsic genetics of androgenetic alopecia.
Treatment depends on what is found. A few broad principles are consistent:
Ultimately, hormones are only one chapter in the hair loss story. They are important, but they sit alongside genetics, immune function, nutritional status and environmental exposures.