Join the Newsletter
Blood tests can be helpful in some types of hair loss, but they are not mandatory for everyone. This article explains when laboratory investigations are likely to change management, which tests are commonly used in different clinical scenarios, when extensive testing adds little value, and some pitfalls to be aware of, including supplement-related interference.
![[headshot]](https://cdn.prod.website-files.com/68207da82e5b8c350c67932f/68c6a7436a552c0fe87a4da7_Screenshot%202024-11-27%20at%2011.38.11.png)
Laboratory tests are not the starting point in assessing hair loss. The sequence is:
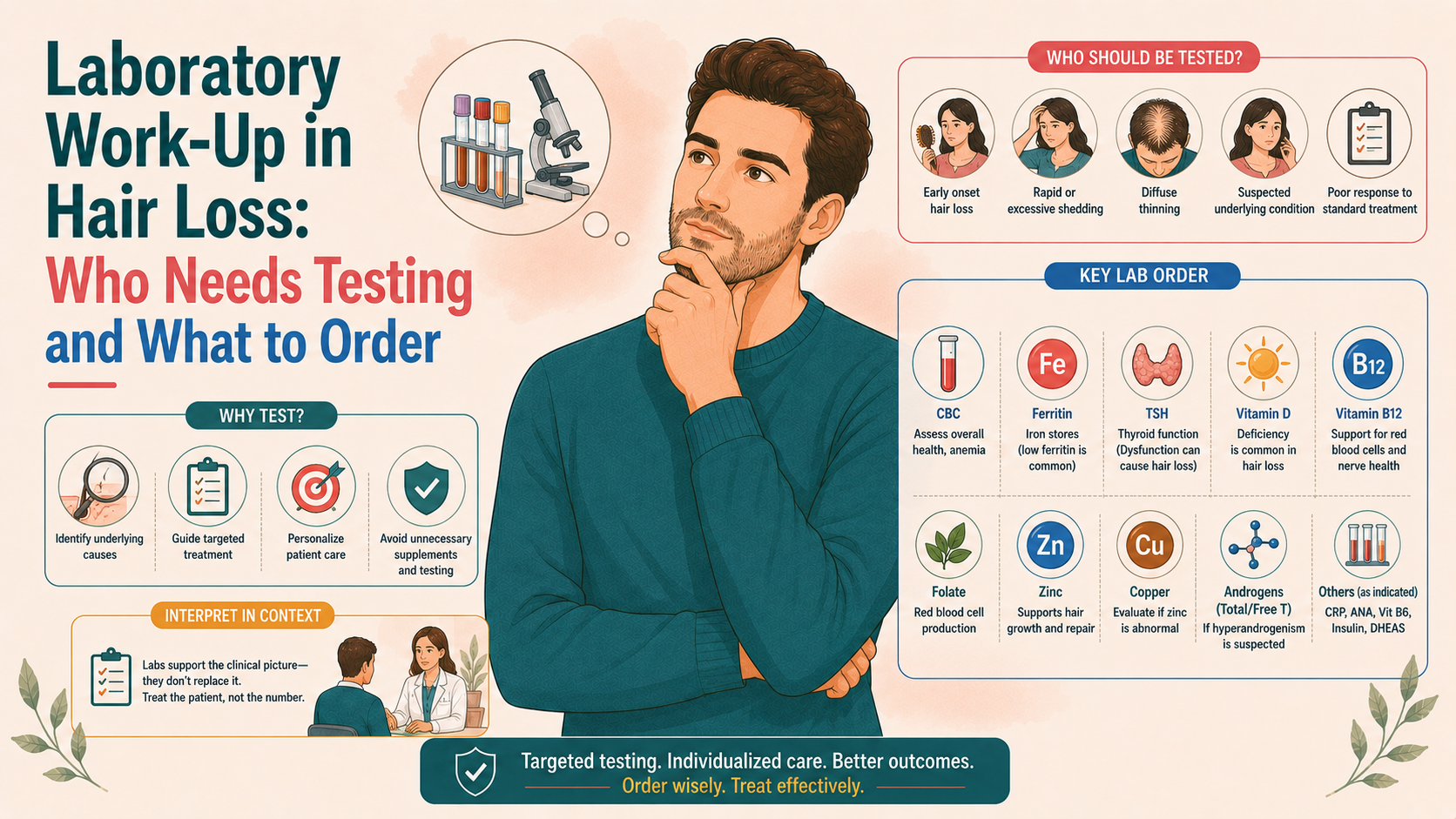
Tests are ordered to:
They are not required to diagnose straightforward androgenetic alopecia in otherwise healthy men, nor should they be ordered as an indiscriminate “full screen” without reference to history and examination.
Guidelines consistently recommend a targeted approach.
In a man with a typical Hamilton–Norwood pattern, normal scalp skin on examination, and no systemic symptoms, most guidelines suggest that a diagnosis of male androgenetic alopecia can be made clinically without routine blood tests.
Similarly, in a woman with classic FPHL (female pattern hair loss, i.e. central part widening and preserved frontal hairline), no signs of hyperandrogenism (hirsutism, acne, or menstrual disturbance), and no diffuse shedding, systemic symptoms, or nutritional red flags, investigation can be limited or omitted, particularly if she is older and otherwise well.
In other words, if the presentation aligns with what is commonly seen in genetically driven hair loss, whether male or female, no laboratory tests are needed. However, if other unaccounted-for medical symptoms accompany the alopecia, tests are indicated.
It is not a black-and-white issue, however, and ultimately comes down to the clinician's judgment.
In ambiguous cases, tests may be considered if there is diagnostic uncertainty, treatment has failed in unexpected ways, or the patient prefers to have a baseline haematological and metabolic assessment. However, routine extensive laboratory testing for every person with pattern hair loss is not supported by the evidence.
In diffuse hair shedding, especially when no clear trigger is present, initial blood work is usually warranted. Typical tests include:
These tests aim to uncover systemic contributors to telogen effluvium rather than to directly diagnose a hair disease.
In women with hair loss and clinical features of androgen excess (e.g. hirsutism, persistent acne, irregular or absent menses), endocrine evaluation is appropriate. This may include:
The aim is to detect or characterise conditions such as polycystic ovary syndrome, non-classic congenital adrenal hyperplasia, or androgen-secreting tumours. Findings guide whether anti-androgen therapy or input from an Endocrinologist is appropriate.
When hair loss coexists with systemic symptoms such as joint pain, fevers, photosensitivity, other skin signs (malar rash, discoid plaques, livedo), then autoimmune screening may be warranted, including but not limited to:
In discoid lupus erythematosus or mixed connective tissue disease, blood tests support the histological and clinical findings. Input from a Rheumatologist is necessary here.
In primary scarring alopecias (lichen planopilaris, frontal fibrosing alopecia, CCCA, discoid lupus, folliculitis decalvans, dissecting cellulitis), blood tests themselves do not diagnose the hair disorder, but may be used to:
A biopsy is required to confirm the diagnosis in these cases, but laboratory testing can help narrow this down. Dermatology input is needed here.
In any patient with hair loss and systemic symptoms such as fatigue, weight changes, night sweats, gastrointestinal disturbances, or lymphadenopathy (swollen glands), a broader work-up may be needed, as these symptoms may suggest anything from chronic infection, liver cirrhosis, an autoimmune process, or even cancer.
It's unlikely that alopecia will be the chief complaint in this scenario, given the severity of the other symptoms. These patients will require hospital admission for workup.
In children, the laboratory work-up is often guided by suspicion of tinea capitis (a fungal infection that requires scalp scrapings or hair plucks for microscopy and culture rather than blood tests), by the presence of systemic signs, and by signs of nutritional deficiency or chronic disease.
Routine extensive blood work for isolated mild alopecia areata in an otherwise well child is not generally recommended in the absence of other autoimmune or systemic clues.
Assesses for anaemia (low red blood cells), thrombocytopaenia (low platelets), or leucopaenia (low white cells), and other haematological (blood-related) abnormalitie.
Anaemia from iron deficiency, chronic disease or B12/folate deficiency can contribute to diffuse shedding.
Ferritin is an iron-storage protein, and thus its levels reflect iron storage, whereby very low ferritin (<15–20 μg/L) strongly suggests iron deficiency.
Some authors recommend aiming for ferritin above 30–50 μg/L in hair loss patients, though evidence for a strict threshold is mixed.
If ferritin is low and there are risk factors (heavy menstruation, gastrointestinal bleeding, vegan diet, malabsorption), iron supplementation and further evaluation may be warranted. Iron studies (serum iron, total iron-binding capacity, transferrin saturation) help confirm the diagnosis.
The thyroid gland, which sits anteriorly in our neck, produces thyroid hormone that drives the metabolic rate of our cells and, by extension, our organs.
TSH (thyroid-stimulating hormone) and sometimes free T4 are used to detect:
Both hypo- and hyperthyroidism can cause diffuse shedding and hair texture changes. Treating the thyroid disorder typically improves hair over several cycles.
Routine high-dose supplementation in the absence of deficiency has not been shown to improve hair growth.
Zinc testing may be considered in patients with a poor diet, gastrointestinal disease, or unexplained diffuse hair shedding.
Severe zinc deficiency is known to cause hair loss, but moderate “low-normal” levels are more difficult to interpret. Excess zinc can impair copper absorption and worsen hair if taken indiscriminately.
Trace elements, such as copper and selenium, are measured selectively, particularly in the context of gastrointestinal surgery, malabsorption, or suspected toxicity.
As noted, in women with suspected hyperandrogenism, an androgen panel can:
Interpretation requires an understanding of assay limitations and should generally be integrated with clinical and ultrasound findings in endocrinology or gynaecology.
In the absence of specific indications, this kind of broad, untargeted testing:
Guidelines and reviews generally advise against:
The principle is that tests should be used when the pre-test probability of a condition is meaningful and when the result would genuinely alter treatment.
High-dose biotin (vitamin B7), often taken for hair and nail health, can interfere with many immunoassays, including those for:
This can produce falsely normal or abnormal results, potentially leading to misdiagnosis. Many laboratories now advise stopping high-dose biotin 48–72 hours before testing; in practice, if a patient takes hair supplements containing biotin, it is important that the lab and clinician are aware of this.
Marginal deviations (for example, slightly low vitamin D, minimally low ferritin, mildly raised ANA) need to be interpreted cautiously:
Avoiding the temptation to equate every borderline result with a causality of hair loss is part of maintaining perspective.
It is common for more than one factor to be present:
Laboratory results need to be interpreted alongside trichoscopy and history. Correcting a deficiency may improve shedding, but underlying pattern hair loss may still need direct treatment.
A tiered approach, broadly consistent with guidelines and reviews, might look like this:
Here, the focus is on clinical diagnosis and treatment options; tests are reserved for atypical features.
Basic tests:
These tiers incorporate endocrine panels, autoimmune screens, and disease-specific tests, guided by history and clinical examination.
From a patient’s perspective, it is reasonable to expect that:
If you feel that your concerns about hair loss are being dismissed without examination, or conversely that you are being over-tested without clear reasoning, it is appropriate to ask for clarification or to seek a second opinion.