Join the Newsletter
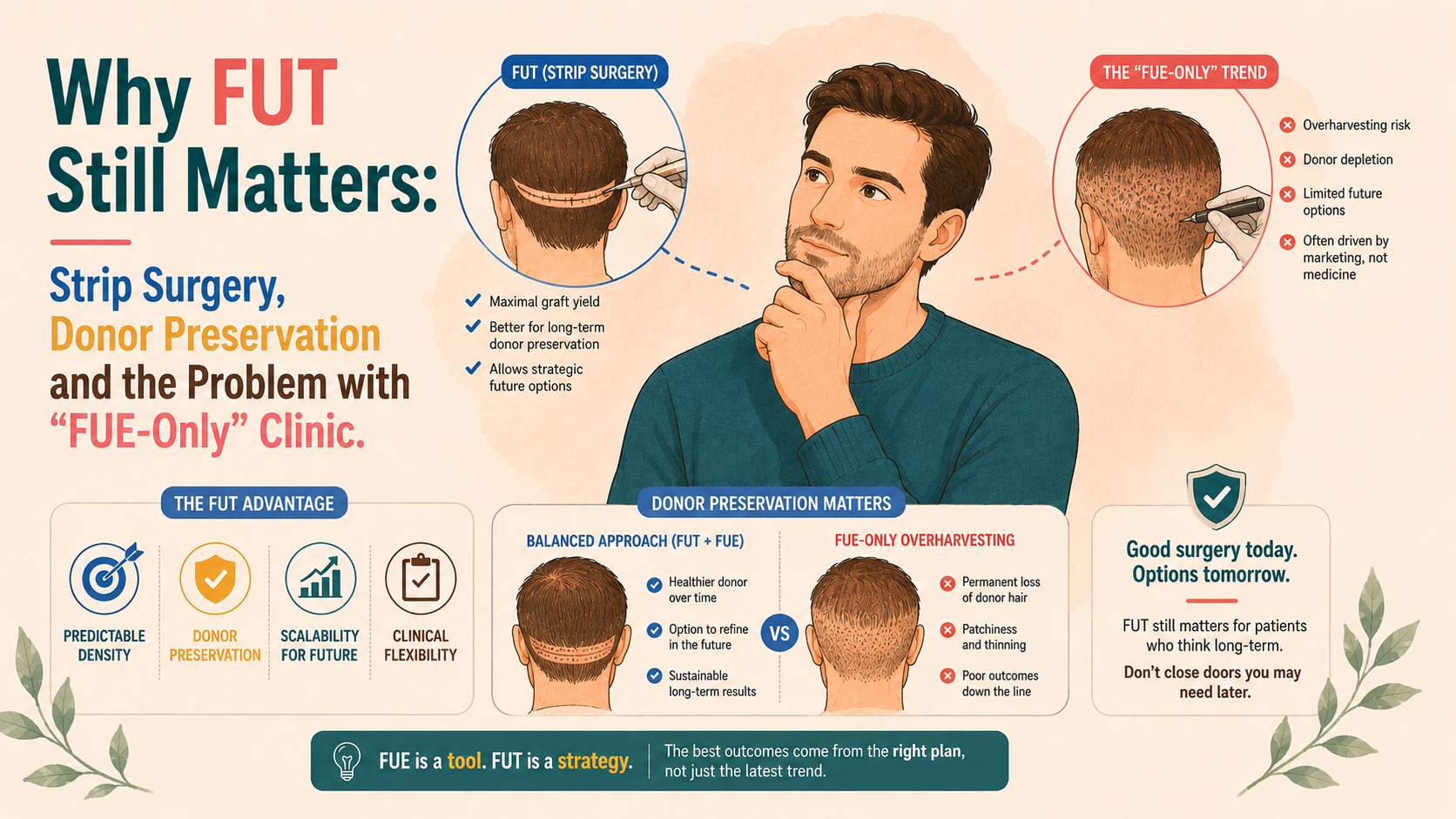
Follicular unit excision (FUE) has transformed hair transplant marketing and made surgery more acceptable to many patients. But in the enthusiasm for “scarless”, “no incision” techniques, a quieter truth is at risk of being lost: follicular unit transplantation (FUT, or strip surgery) remains an important, and in many cases superior, option for donor conservation and lifetime planning. This article explains what FUT offers, how it compares to FUE, why the trend toward FUE-only practices can be problematic, and how patients can ensure they are genuinely being offered the full palette.
![[headshot]](https://cdn.prod.website-files.com/68207da82e5b8c350c67932f/68c6a7436a552c0fe87a4da7_Screenshot%202024-11-27%20at%2011.38.11.png)
Modern hair transplantation is built around follicular units – naturally occurring groupings of one to four hairs that share a sebaceous gland, arrector pili muscle and perifollicular tissue. Whether a surgeon performs FUT or FUE, the implantation side is essentially the same:
The difference lies entirely in how those units are removed from the donor area.
Both techniques, done properly, can yield high-quality grafts and natural results. But their impact on the donor area over the course of a lifetime can be quite different.
Because FUT removes a strip and then microscopically dissects it, it allows:
If a man in his 30s with a strong family history of advanced Norwood patterns is likely to need several thousand grafts over his lifetime, FUT often provides a higher total, dependable graft yield from the permanent zone, with less risk of encroaching on marginal areas that may later thin.
In contrast, FUE disperses the extraction over a broad surface. To match the number of grafts obtained from a single well-planned FUT, a surgeon may need to harvest a high proportion of follicles per square centimetre, with a visible reduction in density if overdone.
FUT produces a single linear scar: in most modern hands, a fine line that can be concealed by hair of even modest length, lying within the permanent donor zone.
For patients who wear their hair longer than a number 3 or 4 guard, this scar is typically invisible in everyday life.
FUE produces multiple small dot scars spread across the donor area. Individually, these dots are insignificant, but collectively, they silently reduce donor density. If the extraction is too dense, it can create a “moth-eaten” look when the hair is cut short.
For some patients, a neat linear scar that can be hidden under hair offers more long-term flexibility than diffuse thinning.
Strip harvesting with microscopic dissection allows:
FUE, particularly when performed at speed or by less experienced teams, has:
Good surgeons can achieve excellent graft quality with FUE, but the technique is more technically demanding to perform consistently at scale.
Importantly, FUT does not preclude later FUE; in fact, it often preserves that option.
A common lifetime strategy is to perform one or more FUTs first, harvest the central, safest portion of the donor, and then use FUE later to fine-tune density, address scars, or supplement coverage once the pattern is more clearly defined.
Starting exclusively with large FUE sessions in a young patient, by contrast, can leave little donor tissue untouched for any future procedure.
The growth in FUE is not arbitrary. It has genuine advantages for certain patients and priorities.
In patients who routinely wear their hair extremely short, are concerned about any linear scar, or have a personal or professional preference for clipped cuts, the ability to distribute dot scars so that no obvious line is visible can be appealing. A well-managed donor area with conservative FUE depletion can look natural even at very short hair lengths.
FUE excels at small “top-up” procedures where only a modest number of grafts are required, harvesting from specific zones (for example, beard or body hair in advanced cases), and camouflaging linear scars from previous FUTs or other surgeries.
For many people, the idea of “no scalpel, no stitch” feels less daunting. Although this is more a matter of language than underlying tissue trauma, it has helped more men and women consider surgery.
The problem is not that FUE is a poor technique. It is that FUE alone is sometimes presented as the only technique, even when FUT would offer important long-term advantages.
In the last decade, several forces have pushed the field towards an FUE-dominant model:
As a result, many clinics now do not offer FUT at all, have surgeons and teams who have never been trained in strip surgery, or present FUE as the default or only surgical option.
For some patients, this is entirely appropriate. For others, particularly young men likely to progress to more advanced patterns, patients requiring a large number of grafts, or those with limited donor resources, being funnelled into FUE-only treatment can be a genuine disservice.
A typical promotional narrative might be:
“We can extract 3,000–4,000 grafts by FUE in a single day, scarless.”
What is not always explained is that:
Without FUT, there is little opportunity to “bank” a large number of grafts from the central permanent zone while leaving the surrounding donor largely intact.
Once dot scars are scattered across the donor and density is reduced, corrective options are constrained:
By contrast, if a man undergoes one or two FUTs and then modest FUE afterwards, there is often more scope to redistribute or refine without exposing the donor.
True informed consent requires that the patient be made aware of both FUT and FUE, that the advantages and disadvantages of each as they apply to their specific case be explained, and that the long-term implications for donor availability be discussed.
An FUE-only clinic, by definition, cannot offer this full menu. The risk is that patients are making decisions based on a partial view of what is possible.
In an ideal world, surgical planning for androgenetic alopecia is done over a timeline of decades, not months. That planning often uses both techniques.
A common, rational sequence might be:
In both scenarios, the strength of FUT is that it respects the donor area by concentrating the unavoidable scar burden into a narrow, concealable zone, leaving most of the remaining donor untouched for future options.
A conversation that properly considers FUT will usually include:
By contrast, a conversation that focuses solely on “scarless extraction”, “no stitches”, or “one big FUE session” without the above elements is incomplete.
You do not need to be a surgeon to ask sensible questions:
If a clinic never mentions FUT, dismisses FUT as “obsolete” without providing a donor analysis, or cannot articulate a long-term plan beyond this year’s FUE, it is reasonable to seek a second opinion from a surgeon who is comfortable with both methods.
FUT is not the right choice for every patient. There are many good reasons to choose FUE as the first or only method. But the idea that strip surgery is inherently outdated, or that its only relevance is in historical textbooks, does not reflect the way many thoughtful hair surgeons still practice.
FUT remains particularly valuable in:
The injustices do not lie in offering FUE, but rather in failing to offer FUT when it is clearly advantageous, or in not being transparent about the fact that it is a clinic’s limitations, rather than the patient’s biology, that determine what is “recommended.”
As with all aspects of hair loss care, the best outcomes come when the full arsenal of tools is on the table, and the choice among them is driven by anatomy, pattern and long-term goals, rather than fashion or convenience. Individualistic planning is constrained when valid options are unreasonably withheld.