1. Why start with the basics?
Almost everyone will experience some degree of hair thinning over the course of a lifetime. For some, it is barely noticeable; for others, it becomes one of the defining health concerns of their adult life. Despite this, many people never receive a clear explanation of what is actually happening in their scalp.
Before talking about specific diagnoses or treatments, it helps to understand the fundamentals: how a healthy hair follicle is built, how it cycles, why those cycles go wrong, and how our interventions try to shift the biology back in our favour.
2. Anatomy of hair and scalp
Each hair on your head grows from a tiny, highly specialised organ: the hair follicle.
The follicle
If you took a cross-section through the scalp, you would see:
- Epidermis: the surface skin layer.
- Hair follicle: a tubular invagination of the epidermis extending deep into the dermis and sometimes into the subcutaneous fat.
- Hair bulb: the enlarged base of the follicle, containing rapidly dividing matrix cells that generate the hair shaft.
- Dermal papilla: a cluster of specialised fibroblasts and blood vessels that sit inside the bulb and act as the “control centre” of the follicle.
- Sebaceous gland: attached to the upper follicle, secreting sebum into the hair canal.
- Arrector pili muscle: a small smooth muscle that can contract to make the hair stand on end.
The hair shaft itself has three main layers:
- Medulla (sometimes absent),
- Cortex, giving the hair most of its strength and bulk,
- Cuticle, the thin outer layer of overlapping cells that protects the shaft.
Follicles are arranged in units, with one to four terminal hairs often emerging from a single visible pore. Their density, size and orientation all contribute to how “thick” or “thin” hair appears to the eye.
3. The hair cycle: how healthy hair grows
Hair follicles do not constantly produce hair at the same rate. Instead, they cycle through distinct phases:
- Anagen (growth phase)
- Lasts several years on the scalp.
- The bulb is active, matrix cells divide quickly, and the shaft elongates.
- In a healthy scalp, 80–90% of follicles are in anagen at any moment.
- Catagen (transition phase)
- A brief “involution” phase lasting a few weeks.
- Cell division stops, the lower follicle regresses, and the dermal papilla moves upwards.
- Telogen (resting phase)
- Lasts roughly three months.
- The old hair remains anchored while the follicle rests.
- Exogen (shedding phase)
- The old hair is released from the follicle and falls out.
- A new anagen hair begins to grow from the same follicle.
There can also be a kenogen interval, where the follicle is empty between shedding and the next anagen phase. In health, this is usually brief; in some hair disorders, it becomes prolonged, contributing to visible thinning.
What matters clinically is the balance and quality of these phases. Hair appears full when:
- Anagen is long,
- Telogen is short,
- Follicles cycle in an asynchronous, mosaic pattern, and
- The shafts are thick, pigmented and emerge at appropriate angles.
4. How common is hair loss?
Hair loss is one of the most common concerns seen in dermatology clinics. Broadly:
- Androgenetic alopecia (pattern hair loss) affects up to 80% of men and around 50% of women over their lifetime.
- Female pattern hair loss becomes more frequent with age, with approximately one-third of women exhibiting some degree of thinning in midlife, and more than half in older age groups.
- Telogen effluvium (reactive shedding) is common after illnesses, childbirth, crash dieting or major stress.
- Alopecia areata affects approximately 2% of the population at some point in life, often in younger individuals.
Scarring alopecia (in which follicles are destroyed and replaced by scar tissue) is less common but clinically significant, requiring early recognition and targeted treatment.
5. Major types of hair loss and their mechanisms
There are many ways to classify hair loss, but a practical starting point is to divide it into non-scarring and scarring forms.
5.1 Non-scarring hair loss
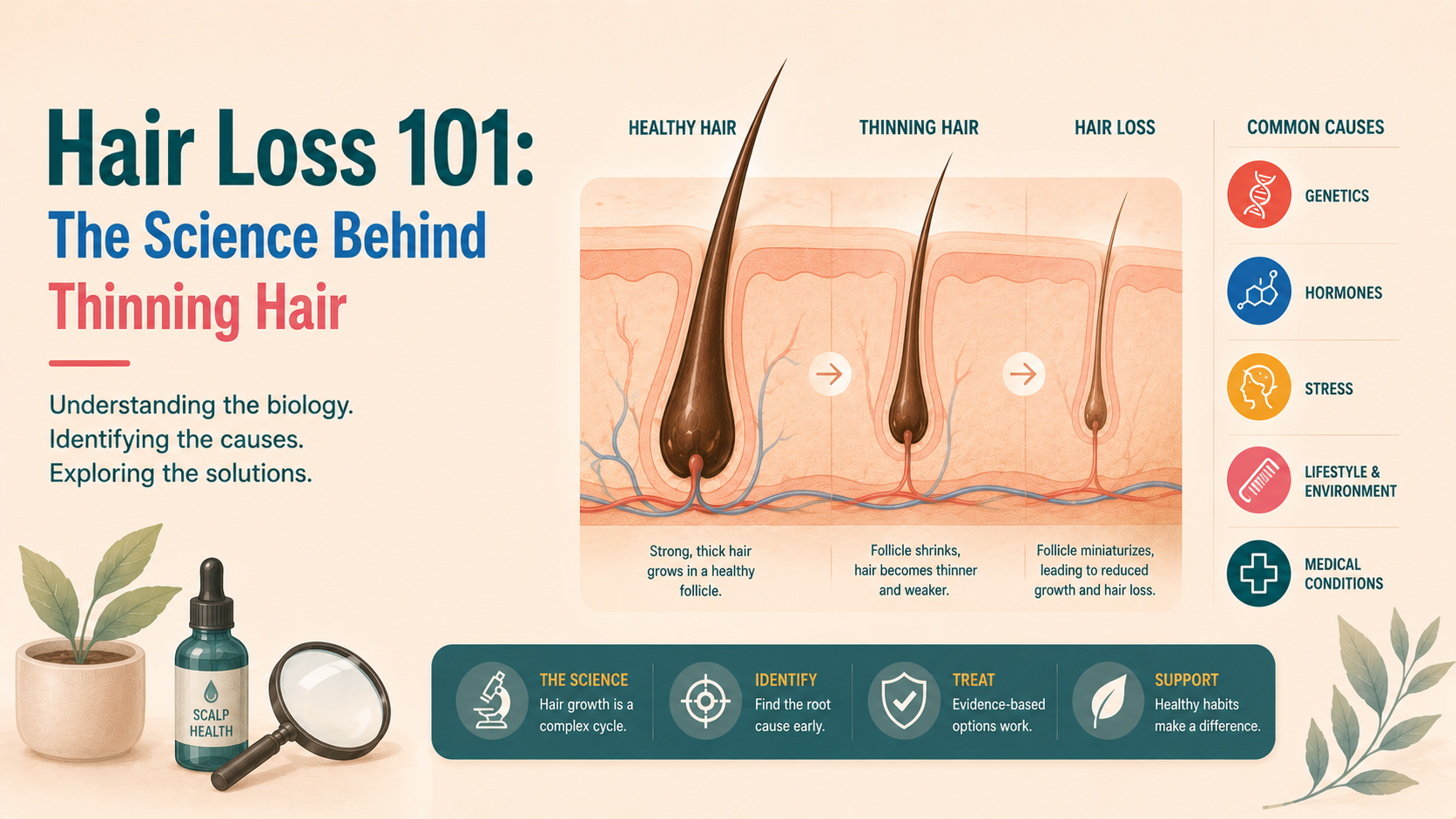
Here, follicles are still structurally present and in principle capable of producing hair, even if they are miniaturised or temporarily inactive.
5.1.1 Androgenetic alopecia (male and female pattern hair loss)
This is driven by genetically determined sensitivity of certain follicles to dihydrotestosterone (DHT), a metabolite of testosterone.
Key features:
- Miniaturisation: susceptible follicles progressively produce thinner, shorter hairs.
- Shortened anagen and relatively longer telogen phases.
- Regional patterning:
- In men, frontal hairline recession and vertex thinning.
- In women, preserved frontal hairline with thinning through the mid and crown.
Not everyone with androgenetic alopecia has high circulating androgen levels. Rather, follicles in certain regions have more active 5-α-reductase, more androgen receptors, or a different response to DHT.
5.1.2 Telogen effluvium
This is a reactive shedding, where a larger-than-normal proportion of follicles shift into telogen simultaneously.
Typical triggers:
- Severe systemic illness or surgery,
- Childbirth,
- Crash dieting or iron deficiency,
- Major psychological stress,
- Certain medications.
Mechanistically, a stressor “resets” the hair cycle, causing many anagen follicles to prematurely enter catagen/telogen. Shedding then occurs a few months later. The follicle is not destroyed; given time and removal of the trigger, regrowth is typically achievable.
5.1.3 Alopecia areata
An autoimmune condition where the body’s own immune system targets the hair follicle, particularly the bulb region in anagen hairs.
Key mechanisms:
- Loss of the hair follicle’s “immune privilege”
- Cytotoxic T-cell infiltration around the bulb,
- Cytokine signalling that halts hair production and pushes follicles into dystrophic catagen.
Clinically, it presents as smooth, sharply demarcated patches of hair loss that may extend to the entire scalp or body.
5.1.4 Traction alopecia and trichotillomania
- Traction alopecia arises when mechanical tension (tight hairstyles, braids, extensions) repeatedly traumatises follicles, especially around the hairline. Chronic traction can transform a reversible state into a scarring process.
- Trichotillomania involves recurrent hair pulling due to an impulse-control or body-focused repetitive behaviour. The mechanical trauma fractures hair shafts and, over time, can damage follicles.
5.2 Scarring (cicatricial) alopecia
In these conditions, the follicular epithelium is destroyed and replaced by fibrous tissue. Once this has occurred, hair cannot regrow from that follicle.
Common examples:
- Lichen planopilaris and frontal fibrosing alopecia - lymphocyte-mediated inflammatory conditions targeting the upper follicle.
- Central centrifugal cicatricial alopecia - often seen in women of African descent, with inflammatory destruction beginning at the crown.
- Discoid lupus erythematosus and other autoimmune conditions involving the scalp.
Mechanistically, these disorders involve aberrant immune responses, interface dermatitis, and subsequent scarring. Early diagnosis is crucial, as timely anti-inflammatory treatment can halt progression, but it cannot restore follicles once they are scarred.
6. The biological basis of current treatments
Understanding the pathology makes it easier to see why our treatments look the way they do.
6.1 Modifying the hair cycle and follicle environment
Minoxidil is the archetypal example:
- It is a potassium channel opener with vasodilatory properties.
- It promotes the conversion of follicles into and retention in the anagen phase.
- It appears to increase local blood flow and VEGF (blood vessel growth factor) levels, thereby supporting follicular metabolism.
Clinically, this translates into longer growth phases, thicker shafts from miniaturised follicles, and more follicles in visible, productive anagen at any one time.
6.2 Modifying androgen signalling
In androgenetic alopecia, the problem is not simply unhealthy hair, but a susceptible follicle in a particular hormonal environment.
5α-reductase inhibitors such as finasteride and dutasteride:
- Reduce DHT levels by blocking the conversion from testosterone,
- Decrease androgenic miniaturising signals to the follicle,
- Allow some miniaturised follicles to produce stronger hairs again.
This fits neatly with the observed biology: regions with the highest 5α-reductase activity and androgen receptor expression respond most strongly to systemic DHT reduction.
6.3 Calming inappropriate immune responses
In alopecia areata and scarring alopecias, inflammation and immune dysfunction become central targets.
- Topical or intralesional corticosteroids reduce the production of inflammatory cytokines and immune cell infiltration.
- Systemic immunomodulators (such as JAK inhibitors in alopecia areata) interrupt specific signalling pathways that sustain the autoimmune process.
- Antimalarials, retinoids, and other agents in scarring alopecias modulate immune function, keratinocyte behaviour, and fibrosis.
Again, the logic flows from pathology: we are not nourishing the hair follicles; rather, we are preventing the immune system from attacking them.
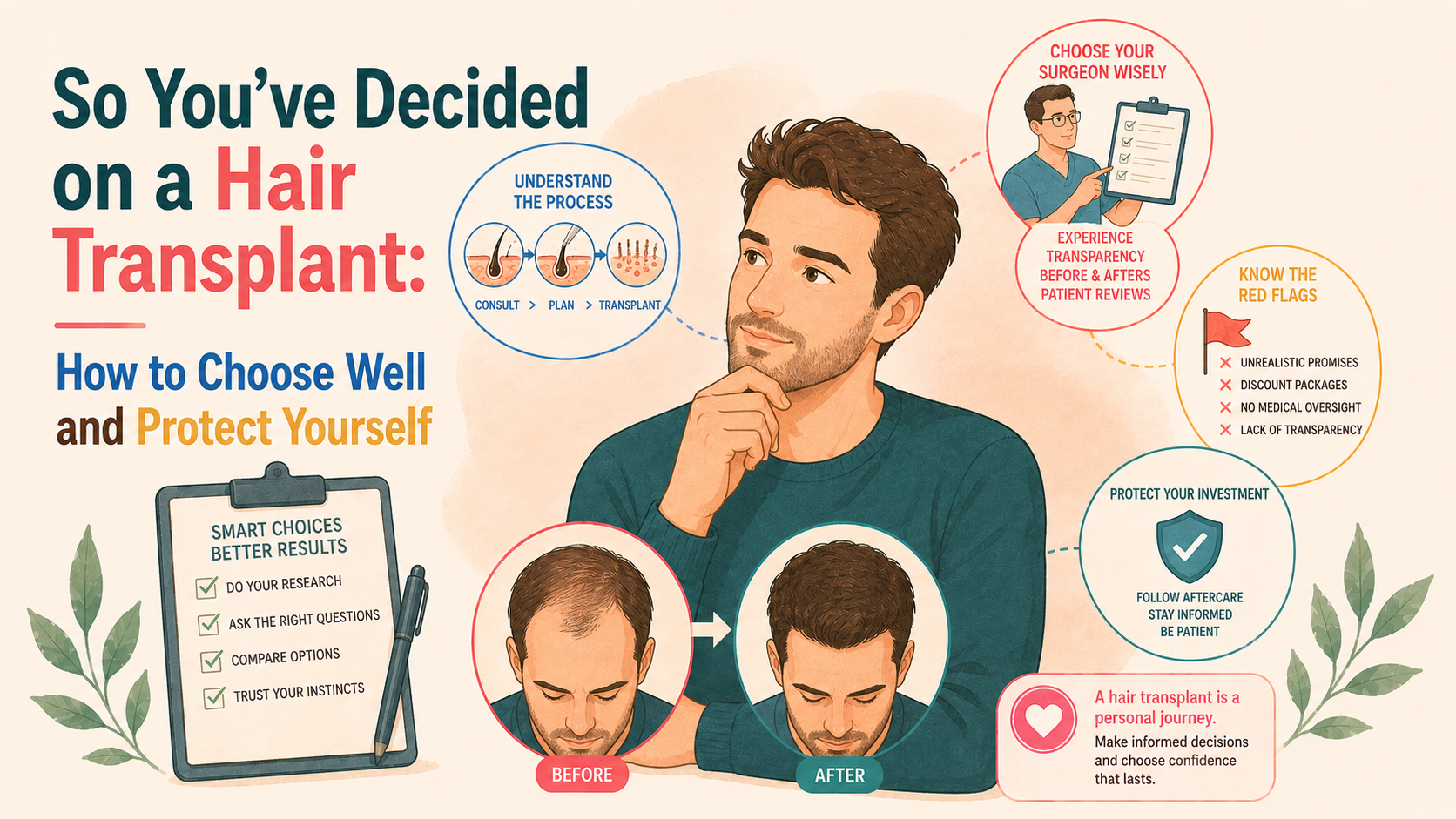
6.4 Physically redistributing follicles
In surgical hair restoration, particularly for androgenetic alopecia, the principle of donor dominance applies:
- Follicles taken from the occipital and parietal scalp are genetically less sensitive to DHT.
- When transplanted into balding areas, they tend to retain their original characteristics and continue cycling as they did in the donor region.
This is not a cure for the underlying predisposition, but a redistribution of relatively resistant follicles to areas where susceptible follicles have been lost.
6.5 Correcting contributory systemic factors
For telogen effluvium and some overlapping scenarios, the “treatment” is often to address an underlying imbalance:
- Replenishing iron stores where ferritin is low,
- Normalising thyroid function,
- Improving nutritional intake,
- Allowing sufficient time for cycles to reset once a stressor is removed.
The biological rationale is straightforward: if many follicles have been simultaneously induced into telogen, removing the stressor and restoring physiological balance allows them to enter a new, more robust anagen.
7. Key messages
- Hair follicles are dynamic mini-organs with their own life cycles; hair loss usually reflects disruption of those cycles rather than “instant death” of the follicle.
- Androgenetic (pattern) hair loss is by far the most common cause, but it is not the only pattern that matters.
- Distinguishing non-scarring from scarring forms and understanding the mechanisms involved are essential for rational treatment.
- Modern therapies are not arbitrary lotions and tablets; they are targeted attempts to interfere with, or support, specific biological processes in the follicle and surrounding skin.
- Early, accurate diagnosis gives you far more room to manoeuvre. Once follicles have been scarred or severely miniaturised for extended periods, options become narrower.
This Knowledge Hub will build on these basics, so that when you read about a specific condition or treatment later, the mechanisms underlying it will feel familiar.

![[headshot]](https://cdn.prod.website-files.com/68207da82e5b8c350c67932f/68c6a7436a552c0fe87a4da7_Screenshot%202024-11-27%20at%2011.38.11.png)